Occasionally, septated uterus are associated with cervical septum and even a vaginal septum. The first case of septated uterus and vagina was published by McBean [McBean JH, Brumsted JR. Septate uterus with cervical duplication: a rare malformation. Fertil Steril. 1994; 62 (2): 415-7.] Since that publication, there have been less tan 300 cases published in the literature..
The presence of double cervix can be associated with different uterine anomalies such as uterus didelphus, bicornuate uterus and septated uterus. The presence of complete septated uterus in cases of double cervix is probably the most frequent association, followed by didelphus uterus, and much less frequent bicornuate uterus. Although a separation of both cervix of more than 1.5 centimeters is more frequent in cases of didelphus uterus, this is not a confirmed rule, and additional diagnostic evaluation must be performed to determine the type of associated malformation [Smith, BC , et al. (2014). “Double cervix: clarifying a diagnostic dilemma.” Am J Obstet Gynecol 211 (1): 26 e21-25.].
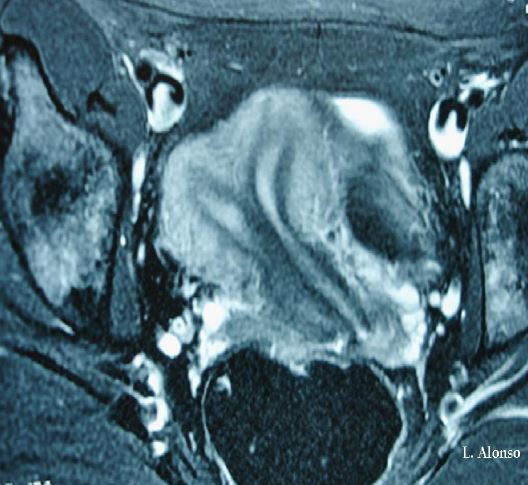
There are several imaging techniques used for the diagnosis of uterine and cervical anomalies, with a different degree of diagnostic accuracy. 2D ultrasound and hysterosalpingography have lower diagnostic accuracy than MRI, which has an accuracy for the diagnosis of Mullerian anomalies between 96-100%. In addition, MRI allows the study of the urinary system, which in some occasions have also associated malformations. 3D ultrasound has similar diagnostic accuracy than MRI.
The largest series published of patients with a complete septated uterus, vaginal duplicity and vaginal septum was reported by Heinonen [Heinonen, P. K. (2006). “Complete septate uterus with longitudinal vaginal septum.” Fertil Steril 85 (3): 700-705.]. In this work, he described the reproductive outcome and clinical implications of septated uterus. This is a descriptive study of 67 patients in which they observed that this malformation was not related to primary infertility and in terms of obstetric outcomes, the spontaneous abortion rate was 27%, the preterm delivery rate was 12% and the newborn alive rate of 72%. Only 4 of these women underwent metroplasty, 3 by hysteroscopy and 1 patient had Jone’s metroplasty.
It is not uncommon to find co-existence of urinary system malformations in these patients. Hainonen reported the presence of renal malformations in 11 patients (20%), being double ureter the most frequent.
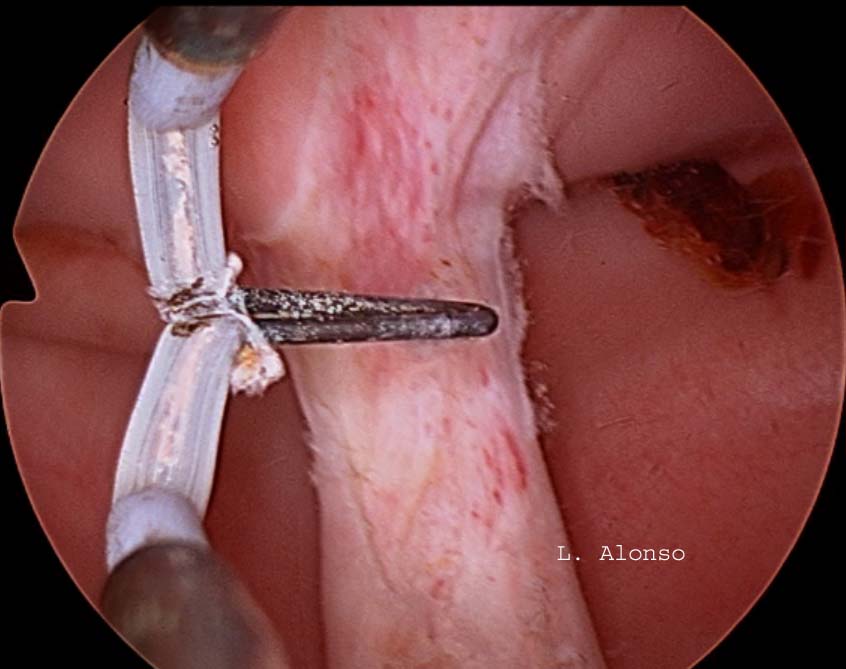
The surgical technique with preservation of the cervical septum was described in a series of 21 patients by Rock [Rock, J.A., et al. (1999). “Hysteroscopic metroplasty of the Class Va uterus with preservation of the cervical septum.” Fertil Steril 72 (5): 942-945.] The description of the technique is as follows: after cervical dilatation, a Foley catheter or a dilator is inserted into one of the cavities that serve as a guide for the section of the body part of the septum. Subsequently, the resectoscope was inserted with a Collin’s loop in the other cavity and the intrauterine septum was incised at the supracervical level.
The arguments favoring to preserve the cervical septum are that it is a vascular structure whose section could result in massive intraoperative bleeding and that the transection of the cervical septum could cause cervical incompetence, which would require performing a cerclage if the patient were to conceive.
The first publication regarding the section of the cervical septum was reported by Vercellini [Vercellini, P., et al. (1994). “A modified technique technique for correction of the complete septate uterus.” Acta Obstet Gynecol Scand 73 (5): 425-428.] Who performed the section of the cervical septum with Metzenbaun scissors in 7 patients in which they had great difficulty in creating the initial communication between the two endometrial cavities. Later, they compared the results of these patients with another group of 9 patients in whom this intracervical septum was left intact. There were no intraoperative or obstetric complications related to the section of the cervical septum. No cerclage was performed on any of the patients.
There are few randomized studies comparing the outcome of excising the entire septum in patients with cervical duplicity. Parsanezhad [Parsanezhad, M.E., et al. (2006). “Hysteroscopic metroplasty of the complete uterine septum, duplicate cervix, and vaginal septum.” Fertil Steril 85 (5): 1473-1477.] compared the results of 28 women with complete uterine septum who had clinical history of poor obstetric outcomes or infertility. The patients were assigned to one of two groups, in one group the intracervical portion of the septum was excised while in the other group the cervical septum was left intact. Both the surgical time and the fluid deficit were greater in the group in which the cervical septum was left intact. In addition, they had two cases of pulmonary edema and 3 cases of massive bleeding in this group. There were no significant differences in obstetric outcomes. 4 of the 15 patients in the group in which the septum was transected had cervical cerclage, whereas it was performed only in 2 of the 13 patients in the group in which the cervical septum was left intact.
In view of these results, the authors recommend transecting the cervical septum in all cases of complete uterine septum, since it makes the procedure safer, faster with similar obstetric obstetrics outcomes.
Further studies are needed to determine the implications that the transection of the cervical septum may have on patients with this rare uterine congenital malformation.
Dr. Luis Alonso Pacheco