Robert’s uterus is a rare uterine malformation of which there are only a few reported cases. In this type of malformation, it is very important to establish a previous diagnosis as well as an appropriate treatment that allows to reconstruct the morphology and functionality of the uterus.
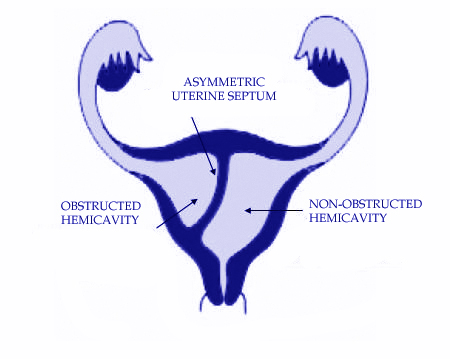
It was first described by Héléne Robert under the name “Asymetrical bifiditis with unilateral menstrual retention”. It is actually an asymmetric variant of the septated uterus and is characterized by having a complete uterine septum that divides the uterine cavity asymmetrically from the fundus up to the Internal Cervical Os (ICO) resulting in a non-communicating hemi-uterine cavity and another hemiuterina cavity with unicorn uterus appearance, all in a uterus with a normal external morphology.
3 types of Robert’s uterus have been described based on the characteristics of the existing hematometra inside the blind hemicavity at the time of diagnosis:
Type I: With gran hematometra
Type II: Without hematometra
Type III: With small hematometra
Usually hematometra and its associated dysmenorrhea are usually of increasing severity over time due to increased tension and size of the blind hemicavity. In cases without hematometra, patients do not usually suffer from severe dysmenorrhea, in these circumstances the most common complaint is recurrent pregnancy loss, since the communicated hemi-uterus behaves like a unicornuate uterus.
Diagnosing this complex Mullerian malformation is difficult resulting in frequent misdiagnosis, often mistaken for a unicorn uterus with a non-communicating rudimentary cavity.
Within the different imaging tests that can be used to establish the diagnosis, 2D ultrasound has low sensitivity, usually misdiagnosing it as unicornuate uterus. Using hysterosalpingography it appears as a fusiform image of the unicorn uterus with visualization of a single fallopian tube.
Magnetic Resonance Imaging (MRI) in the coronal view is the best imaging modality to diagnose Robert’s uterus, demonstrating the uterine septum, the presence of hematomera in the blind cavity and the existence of a normal uterine contour. 3D ultrasound provides similar results to MRI.
The gold standard for diagnosis is the combination of hysteroscopy and laparoscopy that demonstrate a unicorn uterus in the case of hysteroscopy and the existence of a normal morphology of the uterine contour at laparoscopy.
The way to differentiate while performing a laparoscopy a unicorn uterus from a Robert’s uterus is that in Robert’s the uterine contour is normal or with a small indentation of 1 cm while the unicornuate uterus has a greater indentation (Larger than 1 cm).
The only treatment available is surgical, having established two surgical options, on the one hand the realization of a hysterotomy of the dilated hemicavity with drainage of the hematometra, thus avoiding the recurrence. The other surgical alternative is metroplasty with communication of the two hemicavities, this communication can be performed by laparoscopic after hysterotomy of the dilated blind hemicavity or by transcervical route, performing a hysteroscopic metroplasty.
Unfortunately, due to miss-diagnosis and confusion with a non-communicating rudimentary horn, often these patients undergo a total resection of the non-communicating hemiuterus, with the functional impact that comes with such a mutilating procedure.
L. Alonso
Hysteroscopy Newsletter