Experiencing a pregnancy loss could be a traumatic experience for the couple. When recurrent, the sensation of frustration and disappointment acquire their highest level.
It is estimated that 15% of previously confirmed pregnancies will end in a first trimester spontaneous abortion.
Recurrent pregnancy loss is defined by 3 or more consecutive abortions. It is estimated to affects 1% of women. Although there have been attempts to determine predictive factors of abortion, no valid conclusion has been reached. The most common risk factor is the history of a previous abortion [1].
The largest study published on recurrent pregnancy loss revealed that 16% of women would abort again in a subsequent pregnancy after a first
abortion, 25% of women experienced a third consecutive abortion after a second gestational loss and 45% will suffer a fourth abortion after 3 previous gestational losses.
The study of the cause of these abortions has focused mainly on factors such as the presence of thrombophilia, uterine malformations or endocrine alterations. But the most frequent cause is the presence of chromosomal alterations in the embryo.
An abnormal karyotype can be detected in up to 70.3% of abortions with trisomy being the most frequent alteration found (64.6% of cases), followed by triploidies (13.1%) and monosomies X ( 10.4%) [2]
On certain occasions, direct visualization of the embryo can assist in the diagnosis of abortions. Hystero-embryoscopy is a technique described in
1954 by Westin [3], using a 10 mm optic. Subsequently, the studies of J. Ferro and T. Phillip helped to further develop this technique up to the way we know it today. Hystero-embryoscopy offers two main advantages:
1- Direct visualization and morphological study of the embryo: it reveals potential structural anomalies such as neural tube defects, craniofacial or limb malformations in chromosomally normal embryos [4]
2- Direct biopsy of the embryo or chorion: avoiding errors in the diagnosis. According to the study by Ferro et al. maternal contamination occurs in 22.2% of the cases in which the sample is obtained by conventional curettage. [5]
Embryoscopy consists of direct visualization of the embryo inside the uterine cavity between weeks 5 and 8 of gestation. Fetoscopy is the visualization of the fetus after the 8th week of pregnancy [6]. The development of the embryo from its conception to 60 days (8 weeks) is described in 23 stages of embryonic development, called Carnegie stages. This classification is made based on the external morphological characteristics of the embryo and not according to gestational age or embryo size. In fact, two embryos of the same gestational age can be found at different stages of Carnegie, reflecting individual variations in the development of each embryo.
There are 23 stages of Carnegie ranging from when a sperm reaches the egg and gives rise to the zygote until stage 23, which is reached at 60 days and in which the embryo measures about 30 mm becomes a fetus. In this last stage the head is rounded, the eyelids cover the eyes, the tail disappears, and the external genitalia are already formed.
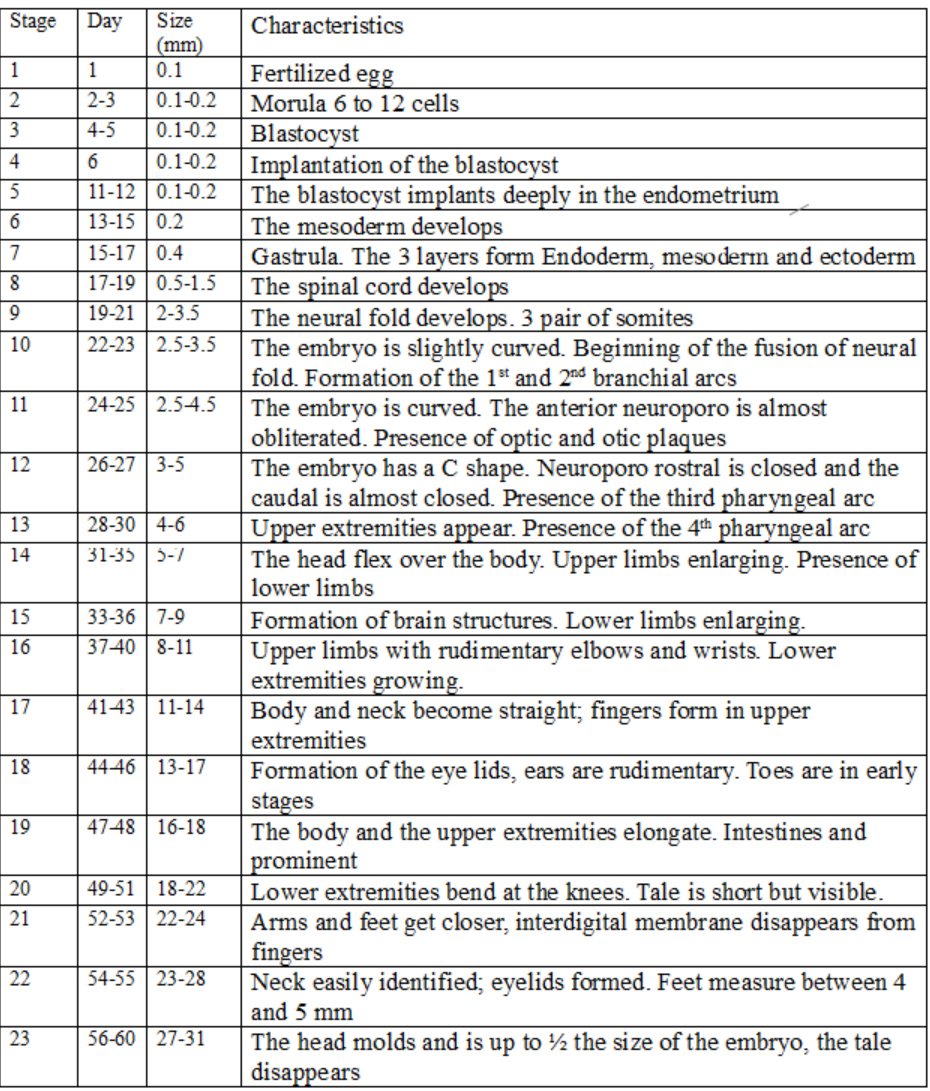
It is important to understand the correlation between the gestational age, the size of the embryo and the morphological characteristics of the embryo. The knowledge of these stages in early phases of the pregnancy is important to determine if there is such a concordance between these characteristics and the expected Carnegie stage.